Women and Smoking: Sensory Factors, Attitudes About Weight, Phase of Menstrual Cycle All Key To Quitting
Download PDF Version What is PDF?
Jill S. Williams
Jill S. Williams is a Contributing Writer for NIDA NOTES.
Source: NIDA NOTES, Vol. 17, No. 4, November, 2002
Public Domain
Table of Contents (TOC)
IntroductionChapter 1: Sensory Factors in Smoking
Chapter 2: Attitudes About Weight Gain
References


NIDA-funded researchers are studying gender differences in smoking behavior and working to develop treatment plans that will help more women end their nicotine addiction. Three recent studies headed by Dr. Kenneth Perkins of the University of Pittsburgh add to this knowledge and test new treatment approaches for women.
In one set of studies, Dr. Perkins has found that the smell and taste of cigarettes play a greater role in women’s smoking behavior than in that of men. Another study found that cognitive-behavioral therapy aimed at changing attitudes about weight promotes smoking cessation by women. Additionally, Dr. Perkins found that menstrual cycle phase has an effect on both mood and tobacco withdrawal symptoms for women trying to quit smoking -- a finding that suggests that women could improve their success rate simply by starting their quit attempt during certain days of their cycle.
Weight Control Methods Impact Smoking Abstinence
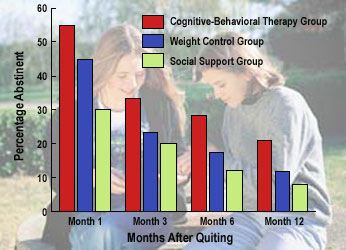
Women who participated in cognitive-behavioral therapy, learning to accept a modest weight gain while trying to quit smoking, achieved greater abstinence levels than those in the weight control group, who were given daily calorie goals, or the social support group, who received counseling that did not focus on weight issues.
Dr. Perkins and his colleagues used a set of laboratory studies to examine the effects of sensory cues -- seeing a lit cigarette and smelling and tasting smoke -- on smoking behavior of women versus men. In one of the studies, researchers recruited 51 young smokers (21 men, 30 women) from the nearby community for what subjects were told was a test of different kinds of cigarettes. The smokers wore opaque goggles or swimmers’ noseclips while smoking to test the roles that visual and olfactory cues -- that is, cues related to seeing and smelling -- play in smoking pleasure and reinforcement. Researchers measured smoking reinforcement -- the number of puffs taken in different situations -- and pleasure -- using subjective measures such as the Rose Sensory Questionnaire -- to assess the extent that sensory cues reinforce smoking.
They found that blocking olfactory stimuli made a greater difference to women than to men. While pleasure in smoking was reduced for both women and men when visual and olfactory cues were blocked, women found significantly less pleasure in smoking and also smoked less than men under the blockade conditions. This study shows that sensory cues play a larger role in smoking for women than for men and further demonstrates that the olfactory cues, not the visual, were the cause of the difference.
 Dr. Perkins has recently tested the effects of nicotine "dose" in
cigarettes on smoking pleasure and reinforcement in 30 men
and women smokers. The smokers sampled, rated, and then
smoked their regular brand of cigarette or an ultra-low-nicotine
cigarette, both of which were presented with brand markings
concealed. The nicotine dose of cigarettes had less effect
on self-reported pleasure and reinforcement in women compared
to men, consistent with the notion that nicotine may be
a less important influence on smoking behavior in women
than in men.
Dr. Perkins has recently tested the effects of nicotine "dose" in
cigarettes on smoking pleasure and reinforcement in 30 men
and women smokers. The smokers sampled, rated, and then
smoked their regular brand of cigarette or an ultra-low-nicotine
cigarette, both of which were presented with brand markings
concealed. The nicotine dose of cigarettes had less effect
on self-reported pleasure and reinforcement in women compared
to men, consistent with the notion that nicotine may be
a less important influence on smoking behavior in women
than in men.
"Because women pay more attention to cues related to smell than do men," says Dr. Perkins, "they could benefit from counseling to avoid those cues and could learn cognitive coping strategies to reduce the urge to smoke." Such behavioral counseling is not now used widely or effectively, he says. He suggests that future research could focus on other conditioned reinforcers of smoking, such as brand markings, "hand-mouth" activity, environmental contexts, and consumption of other drugs (such as caffeine or alcohol), with the goal of finding ways to extinguish the reinforcing effects of these stimuli or finding sensory substitutes.
Dr. Cora Lee Wetherington, NIDA’s Women and Gender Research Coordinator, points out that this study is consistent with other research showing that women may benefit less from the nicotine patch or gum but more from the nicotine inhaler than do men. "Women lose both the sensory cues and the nicotine when they quit smoking," she says. "Therefore, replacing those cues -- something the inhaler can do, but not the patch or gum -- and learning ways to avoid or cope with those cues may help more women succeed in quitting."
Previous smoking cessation trials have found that more than half of women smokers have a hard time quitting, at least partly because of concerns about weight gain. The average postquit weight gain of 10 pounds sabotages many attempts to quit smoking early on and causes some women to resist even trying to quit, to drop out of treatment, or to relapse after quitting. Research has found that dieting to prevent this weight gain is ineffective and may actually interfere with quit efforts. Now, a new study has shown that cognitive-behavioral therapy (CBT) aimed at reducing dietary restraint and changing attitudes about weight proved more successful at both controlling weight gain and promoting smoking cessation.
Dr. Perkins and his colleagues studied 219 women between the ages of 18 and 65 who wanted to quit smoking but were significantly concerned about gaining weight, as determined by telephone interviews during subject recruitment. The women, divided into three treatment groups, all received standard smoking cessation counseling. Each group also received either behavioral weight-control counseling, CBT to reduce weight concerns, or social support not focused on weight issues.
 Members of the weight-control group were given daily calorie goals and instructed
to track food intake in a diary, with the goal of reducing between-meal snacking
(the primary source of excess calorie intake after quitting smoking). These
women successfully prevented any weight gain in the month after quitting,
as expected.
Members of the weight-control group were given daily calorie goals and instructed
to track food intake in a diary, with the goal of reducing between-meal snacking
(the primary source of excess calorie intake after quitting smoking). These
women successfully prevented any weight gain in the month after quitting,
as expected.
The CBT group received therapy to help them accept a modest weight gain in light of the benefits of quitting smoking. In putting together a CBT approach for smokers, Dr. Perkins turned to his colleague Dr. Marsha Marcus, who is an expert on eating disorders. "We wanted to help women accept the likelihood that they may gain 5 to 10 pounds, and we used CBT to modify their attitude toward that weight gain," she says. "We identified unrealistic thoughts or beliefs about weight gain and smoking, and we developed cognitive approaches to counteract those thoughts. Our key message was, ’adopt moderation in eating, reduce stress levels, and exercise more during an attempt to quit smoking.’
At 1-year followup, 21 percent of the CBT group had successfully quit smoking, compared with 13 percent of the weight-control group and 9 percent of the social support group. Weight gain for those continuously abstinent at 1 year averaged 6 pounds for the CBT group, 12 pounds for the weight-control group, and 17 pounds for the social support group.
"Health care providers and smokers should be aware that the CBT approach has more promise than the diet approach," says Dr. Perkins. He suggests that future research can distill the key elements of the CBT intervention so it can be delivered concisely and test a combination of CBT with medication to further improve outcomes.
Today, researchers are paying more attention to the possibility of sex differences and analyzing those differences in their own data. "Both women and health care providers should recognize the obstacles women face and consider how to approach them to maximize their chances of success at quitting smoking," says Dr. Perkins.
Dr. Wetherington sees great value in this type of research: "Because of the gender-based approach Dr. Perkins has taken, we are beginning to see that what works best for males may not work best for females, and vice versa. We are beginning to develop better treatment strategies."
Perkins, K., et al. Sex differences in the subjective and reinforcing effects of visual and olfactory cigarette smoke stimuli. Nicotine & Tobacco Research 3(2):141-150, 2001.
Perkins, K.A.; Jacobs, L.; Sanders, M.; and Caggiula, A.R. Sex differences in the subjective and reinforcing effects of cigarette nicotine dose. Psychopharmocology, in press, 2002.
Perkins, K.A., et al. Cognitive-behavioral therapy to reduce weight concerns improves smoking cessation outcome in weight-concerned women. Journal of Consulting and Clinical Psychology 69(4):604-613, 2001.
Perkins, K.A.; Levine, M.; and Marcus, M. Tobacco withdrawal in women and menstrual cycle phase. Journal of Consulting and Clinical Psychology 68(1):176-180, 2000.
Perkins, K.A. Smoking cessation in women: Special considerations. CNS Drugs 15(5):391-411, 2001.